Today’s Scripture He stilled the storm to a whisper; the waves of the sea were hushed. Psalm 107:29, NIV
He Stills the Storm When you look back over your life, you can see storms of trouble that came against you. Some were bad breaks that had nothing to do with what you had done. Some were unfair, when you were left out or mischaracterized and made to look bad. Other times you tried to step up to a new level, you tried to set a new standard for your family, but opposition you had never faced came out of nowhere. There are forces of darkness that don’t want you to take new ground. When the enemy sees you start to make progress, he’ll send the storm, the waves and the winds, but they cannot stop what God has ordained for you. That’s when God will step up and say, “Peace, be still.” He controls the winds. He has the final say. He pushes back and silences the forces of darkness. What’s come against you is not a sign that you’re stuck; it’s a sign that promotion is coming. You’re about to see things change in your favor, releasing breakthroughs, healing, and abundance to move you into your purpose.
A Prayer for Today “Father, thank You for stilling the storms that are sent to stop my future and for coming to me when the waves were threatening. Thank You that difficulties cannot stop what You have ordained for me. I believe that You are pushing back the forces of darkness and bringing me through. In Jesus’ Name, Amen.”
SECTION TWO
Under the old covenant, it is true that God’s protection was conditional. But for you and me today, it is vital that we read and understand Psalm 91 through the lens of the new covenant—through the lens of the cross.
We are no longer living under the old covenant. We have a new and living way (Heb. 10:20)! Under the old, protection is achieved. Under the new, protection is received.
I have covered the differences between law and grace extensively in my books such as Destined to Reign and Grace Revolution, so I won’t delve too deeply into this subject here. All I really want you to see is this: The cross has made a difference.
At the cross, God “made Him who knew no sin to be sin for us, that we might become the righteousness of God in Him” (2 Cor. 5:21). Today, we are the righteousness of God in Christ!
Because we are righteous in Christ, we can receive the promise of Psalm 5:12, which declares, “For You, O LORD, will bless the righteous; with favor You will surround him as with a shield.”
Naturally, we can’t always watch our backs. But supernaturally, God has got us covered all around. His abundant supply of grace (unmerited favor) encompasses us like a mighty and impenetrable force field, surrounding us 360 degrees and twenty-four hours a day!
Coming back to Psalm 91:14, how do we set our love upon God today? We set our love upon God by meditating on, talking about, and listening to preaching about His love for us!
Remember, it is not about our love for Him, but His love for us. It is about us meditating on Bible verses such as, “For God so greatly loved and dearly prized the world that He [even] gave up His only begotten (unique) Son, so that whoever believes in (trusts in, clings to, relies on) Him shall not perish (come to destruction, be lost) but have eternal (everlasting) life” (John 3:16 AMPC).
There is protection and deliverance from destruction when you believe in God’s love for you. Set your mind on how greatly loved and dearly prized you are. The more conscious you are of the Lord’s love for you, the more His protection will manifest in your life!
The role of Community Pharmacists in TCAM practice by Livy-Elcon Emereonye
According to the World Health Organization, medical practice is classified into three namely: Orthodox or Conventional Medicine, Traditional Medicine (TM), and Complementary and Alternative Medicine (CAM). Natural Medicine is a combination of Traditional Medicine (TM) with Complementary and Alternative Medicine (CAM). In other words, Traditional, Complementary and Alternative Medicine (TCAM) is Natural Medicine.
From the above, one can say that there are basically two types of medicines: Orthodox Medicine and Natural Medicine. An unbiased marriage between the two is what is called Integrative Medicine.
Globally, there is an awakened consciousness in the practice of Natural medicine, and Nigeria is not left out in this trend. The Nigeria land mass with its rich bio-flora and biodiversity are of immense advantage.
The philosophy of Natural Medicine (TCAM) is different from that of Orthodox Medicine. The therapeutic substances used in Orthodox Medicine are called medicines (drugs), but in Natural Medicine therapeutic substances are called remedies. Differences also exist in the methods of production and administration of medicines and remedies.
Whatever the case, the patient is not only the target but the end user of both medicines and remedies. This calls for caution and utmost care. There is a need for standardization and proper regulations.
Natural medicine is not just broad; the opportunities therein are huge and the same goes with the challenges and risks. Thus, the need for adequate training and proper regulation bearing in mind that quacks exist in every practice and errors can occur in every human endeavour. This can be minimized or mitigated with a functional standard operation procedure.
The community pharmacy is the most accessible health facility in the world. Activities in the community pharmacy are geared towards health promotion, disease prevention and therapeutic management through pharmaceutical care. It is the centre for rational drug therapy through incisive drug audit.
A community pharmacy by operation may include a community-based pharmacy traditional retail setting, a retail pharmacy operating out of both large and small chains or grocery stores, an outpatient pharmacy found within a health systems, a federally qualified health centre, a primary care clinic, compounding pharmacy that prepare medications for patients who require unique dosing or modified formulations, and a specialty pharmacy where patients receive outpatient care for complex medication therapies. Whatever the type, the community pharmacist makes the community pharmacy.
The community pharmacist is the most accessible healthcare professional. Among other things, he provides personalized advice about health issues and medicines when needed, sometimes without the need for an appointment, and oftentimes at no cost. A competent community pharmacist is passionate and dedicated to duty with focus on the patient’s wellbeing. This is an opportunity nay a blessing everyone should explore and enjoy without delay or hindrance.
As a drug expert, the primary role of the community pharmacist is to fill prescription, review and detect medication errors as well as recommend and dispense over the counter drugs (OTCs).
The expanded role of a community pharmacist geared towards patient safety include among others to: process prescriptions, check for drug interactions, dispense medications, prepare medications, dispose medications, counsel patients, provide advice, promote healthy lifestyle, and engage in public health programmes.
The roles of a community pharmacist in patient safety has been summarized in
the rights to describe the steps that lead to safe medication use through the right dose of the right medication taken by the right patient at the right time and by the right route for the right indication and right duration. This is the summary of Rational Drug Therapy, and going further, each part of the medication use process may contain different numbers and types of “rights” whose expansion authenticates the indispensable role of the pharmacist in the healthcare team. For example, in the community pharmacy setting, outcomes like the right education, right monitoring, right documentation, and right drug formulation are functions that can only be done properly by the pharmacist, so to safeguard the health of the people, these rights must apply in TCAM remedies.
The marketing, distribution, dispensing, and even administration of TCAM remedies are key areas community pharmacies and the community pharmacist can play a very important role.
Another area where the “trained and certified” Community pharmacist can play important, if not an indispensable role, is in patient counseling.
The monitoring and reporting of possible interactions: remedy-remedy interaction, remedy-food interaction, remedy-drug interaction, as well as adverse events reporting of TCAM remedies are specialized roles of community pharmacists.
The therapeutic role of the pharmacist is required to establish and review standardized dosing information: dosage, frequency and duration for TCAM remedies especially those administered orally with emphasis on pregnant women and children.
Furthermore, the area of Research and Development in TCAM is a gold mine begging to be explored. ACPN and PSN should liaise with Research Institutes and Universities to carry out more research on our “bio-flora”.
The concept and philosophy of “From Farm to Pharmacy (F2P)” should be embraced and maximized by Community Pharmacists. The opportunity therein is huge. The economic and health benefits are endless.
Being the healthcare professional visited most frequently and seen most often by patients and patient relatives, the community pharmacist is in a vintage position to play a vital role in the continued healthcare and check-ups for patients for optimum health through Orthodox or Natural medicines approach using allopathic drugs or TCAM remedies.
As usually, abuse is inevitable where value is not known, and where the right professionals shy away from their responsibilities, charlatans will take over.
Therefore, there is a need for the rational distribution, dispensing and use of TCAM remedies by trained pharmacists in registered premises.
In conclusion, the regulation of the production of TCAM remedies and products should remain with PCN and NAFDAC while TCAM Council when signed into law should regulate the training and practice of TCAM.
Livy-Elcon Emereonye; Pharmacist, Herbalist, Naturopath and Integrative Healthcare Practitioner is the Chairman of ACPN-TCAM Special Interest Group, and PSN TCAM Desk Officer.
We can do training and consultancy on TCAM for interested members.
This is the first post on my new blog. I’m just getting this new blog going, so stay tuned for more. Subscribe below to get notified when I post new updates.
Can I show you a beautiful picture of God’s love for you found in the story of Daniel? In Daniel’s case, the law of the land was violated and, in spite of his love for Daniel, the king had to carry out the law and punish Daniel. If he hadn’t, he would have been an unrighteous king.
Now, imagine if someone came again a year later to accuse Daniel of this crime and asked for Daniel to be punished again, what would the king do? Would the king throw Daniel into the lions’ den again? No! Daniel had already been sentenced; he had already paid the price for his violation of the law.
My dear friend, because our Lord Jesus has been punished on the cross in your place, the devil cannot come to the King and ask for you to be punished and thrown into the lions’ den. You see, your sins were forgiven not because the King simply decided to close an eye and let you off the hook. The King forgave your sins righteously after judging them in the body of our Lord Jesus Christ.
He who was completely without sin took your place and bore the full weight of the punishment for your sins (2 Cor. 5:21). ALL your sins have been legally and judicially judged at the cross. Because of His finished work, once you received the Lord Jesus into your heart, God’s justice and righteousness are on your side!
Do you know how much God loves Jesus, His beloved Son and the apple of His eye? Then I pray that you will have a revelation of how much your Father in heaven loves YOU.
To redeem you, God paid the price with the blood of His only Son. It must have been a most difficult decision for Him. None of us would ever fully comprehend what God experienced in sending His own beloved Son to the cross.
We catch just a small glimpse of the torment that God suffered when we read about King Darius’s suffering. King Darius wanted to save Daniel, but he could not violate his own law.
Similarly, God loves His Son, but He knew the only way to save us, who had violated the law, was to sacrifice His own Son, Jesus Christ. May this revelation of His amazing love and grace give you boldness to come freely to Him and find protection under His wings.
Today’s Word Today’s Scripture “I will give you the keys of the kingdom of heaven; whatever you bind on earth will be bound in heaven, and whatever you loose on earth will be loosed in heaven.” Matthew 16:19, NIV
Bind and Loose We all have things that come against us and try to hinder us and keep us from our destiny. It might be a sickness, depression, an addiction, low self-esteem, or poverty. Sometimes we’re dealing with a dysfunction that’s been passed down in our family line for generations. It’s easy to accept it and think that’s our lot in life, that we’ll always be held back. But God didn’t create you to live restricted, bound, or broken. That may be the way it’s been, but that’s not the way it’s going to stay. The good news is that Jesus came to free you from what’s bound you.
He has already ordained times of release when He looses you from what’s holding you back, when He breaks chains, frees you from the sickness, delivers you from oppression, stops the dysfunction.
Jesus says that whatever you bind will be bound and whatever you loose will be loosed. So get in agreement with Him and bind whatever is hindering you and loose whatever needs to be released. You’re about to come into supernatural release, something you couldn’t make happen.
A Prayer for Today “Father, thank You that Jesus is the chain breaker who frees me from whatever has me bound. Thank You that You have given me the keys of the kingdom to bind whatever is hindering me and to loose whatever needs to be released. I believe this is my time of release. In Jesus’ Name, Amen.”
SECTION TWO
Our enemy the devil is well aware that the moment you learn to receive God’s grace, you will start to reign in life. So he has been working hard to prevent you from receiving the abundance of grace and the gift of righteousness.
The devil has been using controversy as a device down through church history to prevent believers from having access to the most powerful truths of God. He has built fences of controversy around healing, prosperity, and grace (calling them heresies) to keep believers from reigning over sickness, poverty, and sin. You can always tell how powerful a truth is by the number of controversies the devil surrounds it with!
Please pay close attention to what I am saying. Not all controversies are based on the truth of God’s Word. We have to test everything against what the Bible says.
Nevertheless, controversy is a tool that the devil uses to prevent God’s people from accessing His truths. He is a crafty liar and deceitful thief, so we have to base what we believe on the Scriptures and test everything against it. If you want to know the truth about God’s grace, study His Word yourself and see what it has to say about grace!
Pastor Prince, are you one of those “prosperity gospel” preachers?
My friend, there is no such thing as a “prosperity gospel.” There is only one gospel in the Bible—the gospel of Jesus Christ.
However, when you believe the gospel of Jesus, which is based entirely on His grace, it will result in health and abundance of provision. In fact, the gospel of Jesus Christ leads to blessings, success, healing, restoration, protection, financial breakthroughs, security, peace, wholeness, and much more!
God blesses you not because you are good, but because He is good. It is based on His faithfulness and goodness toward you. It is not contingent on your performance, but on His undeserved favor.
If it were contingent on how good you are, then it would no longer be grace but the law. It would be deserved favor. This is the difference between the old covenant of law and the new covenant of grace:
Law is deserved favor—When you obey the commandments perfectly, you will be blessed.
Grace is undeserved favor—Jesus obeyed God perfectly, and you will be blessed by believing in Him.
My friend, which covenant are you under today? Law or grace? Deserved favor or undeserved favor? How do you see God—as your Judge or loving Father?
If you think that being blessed by God today is dependent on your doing, your ability to keep the law, and your ability to make yourself righteous, I ask you to test your understanding of grace against the Scriptures.
Read today’s Scripture again and open your heart to what it says about God and His grace toward you: God is your loving Father in heaven who loves you and has nothing but good gifts for you. He sent His Son to die for you so that you can enjoy every one of these good gifts. Today, receive His abundant grace!
Thrombosis: Causes, Clinical Manifestations, Conventional Management, and Integrative Herbal Medicine Perspectives
By Livy-Elcon Emereonye
One of the main causes of preventable death around the world is blood clots. Being aware saves lives!
Thrombosis remains a leading cause of morbidity and mortality worldwide, underpinning major cardiovascular events such as stroke, myocardial infarction, and pulmonary embolism. It arises from complex interactions between vascular injury, blood flow abnormalities, and hypercoagulability. While conventional management relies heavily on anticoagulant and thrombolytic therapies, increasing attention is being directed toward integrative approaches that include lifestyle modification and evidence-based herbal interventions. This article provides a comprehensive academic review of thrombosis, encompassing its pathophysiology, risk factors, clinical presentation, diagnosis, and management, while critically examining the role of integrative and herbal medicine as adjunctive strategies in thrombosis prevention and long-term vascular health.
Introduction
Thrombosis is a pathological process characterized by the formation of a blood clot within the vascular system, leading to partial or complete obstruction of blood flow. Globally, thrombotic disorders account for a substantial proportion of cardiovascular deaths, with venous thromboembolism (VTE) alone affecting millions annually (World Health Organization [WHO], 2023).
Modern lifestyles—marked by physical inactivity, metabolic diseases, chronic inflammation, and aging populations—have significantly amplified the burden of thrombotic diseases. Although pharmacological interventions have improved outcomes, they are associated with limitations such as bleeding risk, drug interactions, and long-term dependency. Consequently, there is growing interest in integrative approaches that combine conventional medicine with lifestyle, nutritional, and herbal strategies aimed at restoring vascular balance and reducing thrombotic risk.
Definition and Classification of Thrombosis
A thrombus is an intravascular aggregation of platelets, fibrin, and blood cells that forms under pathological conditions. Thrombosis is broadly classified into:
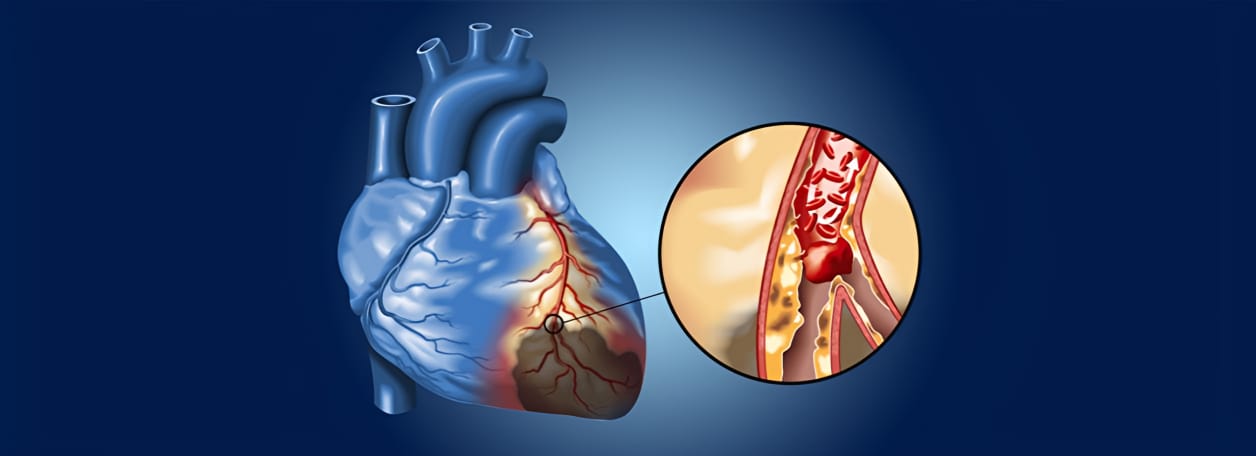
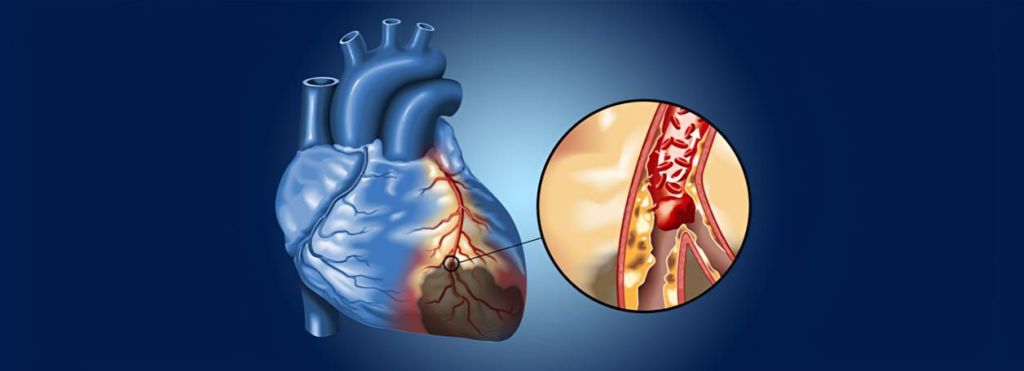
2.1 Arterial Thrombosis Arterial thrombosis typically occurs on ruptured atherosclerotic plaques and is platelet-rich. It is the principal mechanism behind:
Ischemic stroke
Myocardial infarction
Peripheral arterial disease
2.2 Venous Thrombosis
Venous thrombosis is fibrin-rich and commonly manifests as:
Deep vein thrombosis (DVT)
Pulmonary embolism (PE)
Venous thromboembolism represents a major cause of preventable hospital mortality.
Pathophysiology: Virchow’s Triad
The development of thrombosis is classically explained by Virchow’s triad, which includes:
3.1 Endothelial Injury
Damage to the vascular endothelium exposes subendothelial collagen and tissue factor, activating platelet adhesion and the coagulation cascade. Causes include:
Atherosclerosis
Hypertension
Smoking
Surgical trauma
Chronic inflammation
3.2 Abnormal Blood Flow
Stasis or turbulence disrupts laminar flow, facilitating clot formation. This is common in:
Prolonged immobilization
Long-haul travel
Heart failure
Varicose veins
3.3 Hypercoagulability
Hypercoagulable states may be inherited or acquired and include:
Genetic thrombophilias
Malignancy
Pregnancy and oral contraceptive use
COVID-19–related coagulopathy
Chronic inflammatory disorders
Clinical Manifestations
The clinical presentation of thrombosis depends on the affected vascular territory.
4.1 Deep Vein Thrombosis
Unilateral leg swelling
Pain or tenderness
Local warmth
Skin discoloration
4.2 Pulmonary Embolism
Sudden dyspnea
Pleuritic chest pain
Tachycardia
Hemoptysis
Syncope or sudden death in massive PE
4.3 Arterial Thrombotic Events
Stroke: facial asymmetry, hemiparesis, aphasia
Myocardial infarction: chest pain, diaphoresis, nausea, radiation to arm or jaw
Anticoagulants remain the cornerstone of thrombosis management:
Unfractionated heparin
Low-molecular-weight heparins
Vitamin K antagonists (warfarin)
Direct oral anticoagulants (DOACs)
6.2 Thrombolytic Therapy
Reserved for life-threatening cases, thrombolytics actively dissolve clots but carry significant hemorrhagic risk.
6.3 Interventional and Surgical Management
Catheter-directed thrombectomy
Inferior vena cava filters in selected cases
Integrative and Herbal Medicine Perspective
7.1 Rationale for Integrative Approaches
Integrative medicine seeks to address thrombosis not only as an acute event but as a manifestation of systemic vascular dysfunction, chronic inflammation, oxidative stress, and metabolic imbalance. Herbal medicine may contribute through:
Antiplatelet activity
Anti-inflammatory effects
Improvement of endothelial function
Modulation of lipid metabolism
7.2 Evidence-Based Medicinal Plants
Garlic (Allium sativum)
Garlic has demonstrated antiplatelet, fibrinolytic, and lipid-lowering effects. Studies indicate that garlic extracts reduce platelet aggregation and improve endothelial function (Bordia et al., 1998; Rahman & Lowe, 2006).
Ginger (Zingiber officinale)
Ginger inhibits thromboxane synthesis and platelet activation, offering mild antithrombotic effects (Verma et al., 1993).
Turmeric (Curcuma longa)
Curcumin exhibits anti-inflammatory and anticoagulant properties through inhibition of platelet aggregation and modulation of inflammatory pathways (Aggarwal & Harikumar, 2009).
Ginkgo (Ginkgo biloba)
Ginkgo improves microcirculation and reduces platelet-activating factor activity, making it relevant in cerebral and peripheral vascular disorders (Smith et al., 1996).
Omega-3 Fatty Acids
Although not herbal in origin, omega-3s from plant and marine sources reduce platelet aggregation and systemic inflammation (Mozaffarian & Wu, 2011).
7.3 Safety and Clinical Integration
Herbal interventions should be regarded as adjunctive, not substitutes for anticoagulant therapy. Potential interactions—especially with warfarin and DOACs—necessitate professional supervision. Standardization, dosage regulation, and pharmacovigilance remain essential.
Prevention and Lifestyle Integration
An integrative thrombosis prevention strategy includes:
Regular physical activity
Anti-inflammatory diets
Weight management
Smoking cessation
Stress reduction
Adequate hydration
These measures align with both conventional preventive cardiology and traditional holistic health systems.
Conclusion
Thrombosis is a multifactorial vascular disorder with profound public health implications. While conventional pharmacotherapy remains indispensable, integrative and herbal medicine offers promising complementary strategies aimed at prevention, vascular protection, and long-term health optimization. A scientifically grounded, patient-centered integrative model—anchored in evidence, safety, and interdisciplinary collaboration—represents a sustainable future direction in thrombosis management.
References
Aggarwal, B. B., & Harikumar, K. B. (2009). Potential therapeutic effects of curcumin. International Journal of Biochemistry & Cell Biology, 41(1), 40–59.
Bordia, A., Verma, S. K., & Srivastava, K. C. (1998). Effect of garlic on platelet aggregation. Prostaglandins, Leukotrienes and Essential Fatty Acids, 58(4), 257–263.
Mozaffarian, D., & Wu, J. H. (2011). Omega-3 fatty acids and cardiovascular disease. Journal of the American College of Cardiology, 58(20), 2047–2067.
Rahman, K., & Lowe, G. M. (2006). Garlic and cardiovascular disease. Journal of Nutrition, 136(3), 736S–740S.
Smith, P. F., Maclennan, K., & Darlington, C. L. (1996). Ginkgo biloba extracts for cognitive impairment. Journal of Ethnopharmacology, 50(3), 131–139.
Verma, S. K., Singh, M., Jain, P., & Bordia, A. (1993). Effect of ginger on platelet aggregation. Indian Journal of Medical Research, 98, 240–242.
World Health Organization. (2023). Cardiovascular diseases (CVDs): Fact sheet. WHO.
Today’s Word Today’s Scripture Am I now trying to win the approval of human beings, or of God? Or am I trying to please people? If I were still trying to please people, I would not be a servant of Christ. Galatians 1:10, NIV
Healthy Boundaries
It’s easy to go through life trying to please others out of guilt and pressure. A relative or friend will get upset and have their feelings hurt every time we don’t do what they want. They use control and manipulation to get their way. They expect us to perform, to be there every time they call, to make sure they’re taken care of. If not, they try to make you feel guilty as though it’s your job to keep them fixed, happy, encouraged, and entertained. But here’s a key: You are not responsible for other people’s happiness. You are responsible for your own happiness. Take that pressure off. If you continue to give in, you’ll not have the time and energy for your dreams, and you’ll enable their dysfunction. As long as they have you, they don’t have to change.
You have to set some healthy boundaries, or you won’t have healthy relationships. You have to be strong enough to say, “I refuse to be manipulated by others into trying to meet their demands and fix them. I am not responsible for their happiness.”
A Prayer for Today “Father, thank You that You did not make me to fix other people and try to please them by fulfilling their wishes and demands. I want to be loving and kind and help others who are in real need, but help me to be bold and set healthy boundaries with those who would manipulate and control me. In Jesus’ Name, Amen.”
SECTION TWO
Let me now encourage you with a praise report on the power of praying and speaking Psalm 91 over our loved ones. This came from Brenda, who lives in Connecticut:
My twenty-four-year-old son, Lee, was crossing the street on a crosswalk in New York City when he was struck by a cab on the leg and thrown onto the hood of the car before landing on the street. Miraculously, he was totally fine after the accident! He did not have a single broken bone, bruise, or even a scratch.
I recall that just a few days before the accident, we were having a wonderful time celebrating Thanksgiving. Suddenly, I saw in my mind an image of Lee on a slab and dead in a morgue. I immediately dismissed that image, proclaimed that my son would live and not die, and pleaded the blood of Jesus over him.
I didn’t tell anyone what I’d seen, but just thanked God for His protection for my son and all my family members in Jesus’ name. The morning of Lee’s accident, I also felt led to pray God’s protection over my children from car accidents—not something that I usually do.
Then, later that afternoon, I received a text from Lee telling me about the accident and that he was unharmed. After hearing my son was fine, I got on my knees and cried tears of joy, thanking my wonderful Father God! I am so thankful that the Holy Spirit warned me before the accident happened so I could pray for his protection.
My son had just been awarded an awesome position in his company and we were all celebrating his wonderful new title and how God had opened up doors of favor for him. The accident happened just one day before he started his new job.
At the time I learned about Lee’s accident, I was just listening to Joseph Prince’s message on Psalm 91. I used to pray it over my family all the time, but over the years, I had forgotten about this powerful psalm.
I am thankful to Joseph Prince for reminding me of the power of Psalm 91. When we pray the Word of God over our children or any situation, we release His angels to work on our behalf.
Our God is such a good God, isn’t He? I trust that you are beginning to see how important it is to invest your time in getting His living and powerful Word into your heart, praying it over yourself and your loved ones, and speaking it out loud. Lol aa
Today’s Word Today’s Scripture Yet you, LORD, are our Father. We are the clay, you are the potter; we are all the work of your hand. Isaiah 64:8, NIV
In the Process It’s easy to get down on ourselves because we’re not as far along as we want to be. We focus on our flaws, our shortcomings. Some people live with this nagging feeling inside, telling them something is wrong with them and how they don’t measure up. We put all this pressure on ourselves to change. “I have to be more disciplined…watch my mouth…be a better mother…a better spouse…a better employee.” But God is our potter. He controls the process of changing and shaping you, the when and how fast. The key is to accept yourself while God is in the process.
You’re not supposed to go through life being against yourself, overanalyzing your faults. Focusing on your weaknesses doesn’t help you improve. All that does is slow down the process. It’s good to want to improve, to strive for excellence and grow, but don’t get frustrated if it’s not happening as fast as you’d like. Only God can change some things. Until He gives you the grace to do it, accept yourself where you are. It takes maturity to have peace in the process.
A Prayer for Today “Father, thank You that You are the potter and I am the clay. Thank You for where I am right now, faults and all, and that You hold me in Your hands and are molding and making me. Help me to stop being against myself and to simply trust You with the process for further change. In Jesus’ Name, Amen
Some people think that when they worship God, they are giving something to Him. On the contrary, I believe that as we worship and praise Him, He is giving to us, imparting His life, wisdom, and power into our lives, renewing our minds and physical bodies as well in His sweet presence.
SECTION TWO
Worship is simply a response on our part to His love for us. We don’t have to, but when we experience His love and grace in our lives, we want to. It’s a response birthed out of a revelation in our hearts of just how great, how awesome, how majestic, and how altogether lovely our Lord and Savior truly is.
As we worship Him and become utterly lost in His magnificent love for us, something happens to us. We are forever changed and transformed in His presence. All fears, worries, and anxieties depart when Jesus is exalted in our worship.
We have seen this demonstrated through a worship collection, A Touch of His Presence (Volumes 1 and 2), that we compiled from spontaneous worship songs that flowed from my spirit during intimate times of worship when we simply occupied ourselves with the person of Jesus.
I would sing out what God was putting in my heart, and He would manifest His loving presence. That’s when the gifts of the Spirit would operate and healings would break out among the people in the congregation.
We received a letter from Emma in Germany who said, “Whenever the devil tries to attack me with symptoms of a disease, I would listen to these worship CDs and worship Jesus, my Lord, my Savior, and my Redeemer. I would also often partake of the Holy Communion while listening to the worship songs. After a few minutes, all the symptoms would disappear!” Another brother described how this worship music freed him from paralyzing, irrational fear and chronic sleep problems.
I share these testimonies with you because I believe that some of you want to worship God, but you may not know where to begin when you are alone at home. If that sounds like you, then start by getting ahold of anointed Christian music that can fill your room with the presence of the Lord.
Allow the music to simply wash over you like rivers of living waters. Let His presence flush out every fear and every anxiety. Let His love take away the cares that burden you. Let Jesus be magnified and glorified, and watch Him turn all things around for your good!
LAGOS INTENSIFIES DRIVE FOR SAFE BLOOD AS LSBTS TAKES VOLUNTARY DONATION CAMPAIGN TO RESIDENT
The Lagos State Government has renewed its push to secure a safe, adequate, and sustainable blood supply with the Lagos State Blood Transfusion Service (LSBTS) Voluntary Blood Donation Awareness and One-to-One Sensitization Campaign held on Tuesday, January 13, 2026, at the Lagos State Government Secretariat Community, Alausa-Ikeja.
The campaign, themed “Voluntary Donors, Sustainable Blood: Securing Lagos State’s Blood Supply,” formed part of activities marking the LSBTS Blood Awareness Month and underscored the state’s sustained efforts to promote a culture of voluntary, non-remunerated blood donation among residents.
Declaring the event open, the Commissioner for Health, Prof. Akin Abayomi, said Lagos, with an estimated population of about 30 million people, requires between 200,000 and 250,000 units of blood annually to meet its healthcare needs, stressing that voluntary donation remains the safest and most sustainable source.
Prof. Abayomi disclosed that the state recorded about 141,000 units of blood in the last cycle; approximately 70 per cent of the target, commending Lagosians who voluntarily donated blood and save lives in times of medical emergencies.
He described blood as a “liquid organ,” emphasizing that blood transfusion is comparable to organ transplantation and must therefore follow strict scientific protocols, including rigorous screening and precise donor-recipient matching, to prevent complications and transfusion-related infections.
Professor Akin Abayomi, Commissioner For Health Lagos State & Some Health Officials @ Alausa Secretariat
The Commissioner reassured residents that blood donation poses no health risk to eligible, healthy donors, urging especially young people to make blood donation a regular habit, noting that every pint donated translates directly into lives saved across the state’s health facilities.
Also speaking, the Special Adviser to the Governor on Health, Dr. (Mrs.) Kemi Ogunyemi, said the demand for blood is constant and cuts across emergencies such as childbirth complications, road traffic accidents, surgeries, and other critical medical conditions that occur daily.
Dr. Ogunyemi noted that the administration of Governor Babajide Sanwo-Olu has modernized blood transfusion services in Lagos through digitization, improved tracking systems, and strengthened safety protocols to guarantee that only screened and safe blood is made available to patients.
She stressed that not all prospective donors are accepted, explaining that robust screening processes are in place to protect both donors and recipients, while continuous training of laboratory and transfusion personnel ensures adherence to global best practices.
Reiterating that blood donation is a daily necessity and not a seasonal activity, the Special Adviser called on residents to overcome fears and myths surrounding blood donation, assuring that public confidence remains central to sustaining the state’s blood supply.
In her remarks, the Permanent Secretary, Lagos State Ministry of Health, Dr. Dayo Lajide, commended the LSBTS and voluntary donors for their commitment, describing blood as life and a critical resource that underpins effective healthcare delivery.
Dr. Lajide noted that blood demand often spikes during festive periods due to increased mobility and accidents, but emphasized that the need persists throughout the year, making continuous donation campaigns essential for health system resilience.
Earlier, the Executive Secretary of LSBTS, Dr. Bodunrin Osikomaiya, decried the persistent myths and misconceptions that discourage blood donation in Nigeria, even as medical emergencies, deliveries, and accidents continue unabated every day.
Dr. Osikomaiya explained that the campaign was designed to take advocacy directly to the community, beginning with government offices, MDAs, and public spaces, as part of efforts to lead by example and stimulate wider public participation.
Dr. Osikomaiya & Some Participants
She disclosed that LSBTS is strengthening one-on-one sensitization this year to address individual concerns, while opening its facilities to the public to improve transparency around blood collection, testing, processing, and storage.
The Senior Special Assistant to the Governor on Health, Dr. Oluwatoni Adeyemi, said the campaign also aligns with global blood donation advocacy, noting that LSBTS has expanded digital platforms to enable residents easily access information on where and how to donate blood year-round.
Dr. Adeyemi urged collective responsibility in safeguarding Lagos State’s blood supply, stressing that blood donation should be a continuous civic duty rather than a one-off activity tied to specific campaigns.
Dr. Osikomaiya & Dr Kemi Ogunyemi S.AHealth
Highlighting the human impact of voluntary donation, a donor, Mohammed Asalejo said he has been donating blood since 2022, adding that the experience has improved his sense of well-being and inspired him to encourage others to donate.
Another donor, Alhaji Oladele Asalejo, who has donated blood for over 15 years, described blood donation as beneficial both medically and socially, urging residents not to shy away from donating, as it promotes personal health while saving lives.
The event featured awareness talks, donor mobilization, voluntary blood donation, extensive one-on-one sensitization and pasting of information stickers on cars, with participation from key officials of the Ministry of Health and LSBTS staff, as Lagos State intensifies efforts to secure a reliable and safe blood supply for its growing population.
Today’s Word Today’s Scripture “I am the LORD, and when it is time, I will make these things happen quickly.” Isaiah 60:22, NCV
It Can Happen Quickly When we look at the dreams we want to accomplish and problems we’re hoping will turn around, it can seem like it’s going to take a long time—years to get out of debt, years to recover from a sickness, years to see your business grow. But God doesn’t always follow a normal timeline. He says, “When the time is right, I will do it quickly.” He knows how to speed things up. He knows how to accelerate your dreams, accelerate your healing, accelerate what you’re believing for. He has fast-forward moments of favor coming your way when He will catapult you ahead.
This is why you can’t judge your future based on the progress you’ve seen in the past. Everything seems routine. You’re going along at the same pace and making the same progress. Then out of nowhere, one good break, one contract, one door opens, and you’re suddenly twenty years down the road. Suddenly you’re in management, suddenly you break the addiction, suddenly a relationship is restored. You didn’t see it coming, and you can’t explain it. It’s God accelerating things, propelling you forward.
A Prayer for Today “Father, thank You that You have fast-forward moments of favor with breakthroughs that change what has seemed unchangeable. Thank You that You’re orchestrating what You’ve ordained for my life to be fulfilled. I believe that You will make quick work of what could take years. In Jesus’ Name, Amen.”
When Jesus was crucified on the cross, not only did He wash away all your sins with His precious blood, but He also gave you His very own righteousness as a gift (2 Cor. 5:21). Do you know that you can never lose this righteousness? Your righteousness is a gift from Jesus because it is entirely dependent on His perfect performance and His perfect obedience, not yours.
So my friend, because you are forever righteous in Christ, God hears your prayers every time you pray. Apostle James tells us that the earnest prayer of a righteous man—that’s you—”produces wonderful results”. Not just plain results, but wonderful results!
What provision do you need today, righteous one? Favor for an interview, wisdom to clear your debts, healing for your children? As a righteous man or woman of God, boldly ask Jesus for what you need in prayer!
Being text of lecture delivered at 2026 Annual Convention of 1992 Set, PCC Ihioma
By Livy-Elcon Emereonye
Iivinus E
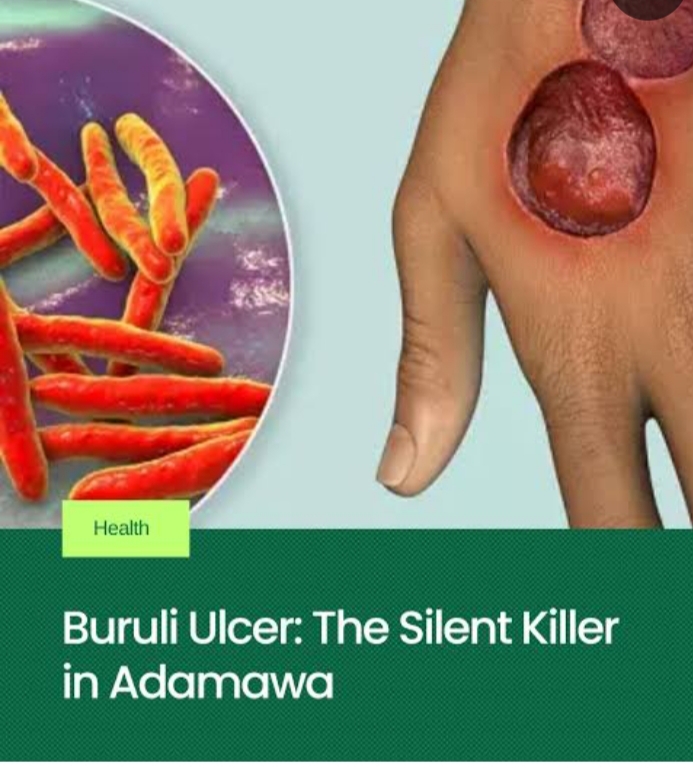
Buruli ulcer (BU), locally referred to in parts of Igboland as Achaere, is a neglected tropical disease caused by Mycobacterium ulcerans. Despite effective antibiotic regimens recommended by the World Health Organization (WHO), delayed presentation, sociocultural interpretations, and inappropriate traditional interventions continue to fuel high morbidity, deformity, and disability in endemic regions.
An Integrative Medicine Approach to the Management of Achaere (Buruli Ulcer)
Introduction
Among the most severe but least addressed neglected tropical diseases (NTDs) is Buruli ulcer. Ranked after tuberculosis and leprosy among mycobacterial infections, BU disproportionately affects rural populations in West and Central Africa, including Nigeria, Ghana, Côte d’Ivoire, and Cameroon. In endemic Nigerian communities, particularly among the Igbo, the disease is colloquially known as Achaere, a term that often carries cultural, spiritual, or metaphysical interpretations.
These interpretations, though culturally meaningful, frequently delay biomedical intervention. Patients often present late, with advanced ulcers, secondary infection, bone involvement, and irreversible disability. At the same time, African traditional medicine remains the first line of care for many rural populations due to accessibility, affordability, and cultural trust.
This reality necessitates not a dismissal of traditional medicine, but a critical scientific engagement with it. The goal of this review is to examine medicinal plants traditionally used for Achaere, evaluate their evidence base, and propose a rational integrative framework that aligns ethnomedical knowledge with modern infectious disease management.
Epidemiology and Public Health Significance
Buruli ulcer is endemic in over 33 countries worldwide, with Africa accounting for the vast majority of cases. Children under 15 years constitute a significant proportion of patients, although adults are also affected. The disease is closely associated with riverine and swampy environments, agricultural activity, and limited access to healthcare.
In Nigeria, underreporting remains a major challenge. Many cases never reach hospitals, instead being managed in traditional settings until complications arise. This contributes to the perception that BU is incurable or spiritually driven, further entrenching harmful treatment practices.
Etiology and Pathophysiology
3.1 Causative Agent
Buruli ulcer is caused by Mycobacterium ulcerans, an environmental mycobacterium distinct from M. tuberculosis and M. leprae. Its unique pathogenicity lies in its production of mycolactone, a lipid toxin.
Mycobacterium ulcerans are rod-shaped, Gram positive bacteria that grow slowly, forming small transparent colonies after four weeks when viewed on a microscope.
Mosquitoes and other aquatic insects (like water bugs) are the primary vectors transmitting the ulcer-causing bacteria Mycobacterium ulcerans from the environment to people.
3.2 Role of Mycolactone
Mycolactone is a nasty toxin:
Induces apoptosis of skin and subcutaneous cells leading to ulcers and tissue damage.
Suppresses local immune responses
Explains the painless nature of early lesions
As a result, patients often ignore early nodules or plaques until extensive tissue destruction has occurred.
3.3 The Role of Immunity
In Buruli ulcer, immunity plays a crucial role:
The disease often affects people with weakened immune systems.
Research suggests that a strong cell-mediated immune response is key to controlling M. ulcerans infection.
Mycolactone suppresses the immune system, making it harder for the body to fight the infection.
Early treatment and a healthy immune system can improve outcomes.
Clinical Presentation
4.1 Early Lesions
Painless nodules
Firm plaques
Diffuse, non-pitting edema
4.2 Advanced Disease
Large ulcers with undermined edges
Necrosis of skin and subcutaneous tissue
Secondary bacterial infection
Osteomyelitis
Deformity and contractures
Pain typically appears late, often signaling secondary infection rather than primary disease activity.
WHO-recommended treatment consists of 8 weeks of combination antibiotic therapy, usually:
Rifampicin + Clarithromycin
This regimen achieves cure rates exceeding 90% when initiated early.
(or Rifampicin + Streptomycin in some settings)
Wound Care
Regular sterile dressing
Debridement of dead tissue
Skin grafting in advanced cases
Physiotherapy to prevent deformities
Psychosocial support.
Surgery
Reserved for large or complicated ulcers
Used alongside antibiotics, not alone
The Place of Traditional Medicine in Achaere
In many African communities, traditional medicine is not an alternative but the default healthcare system. However, in the context of Buruli ulcer, certain practices—scarification, caustic herbal pastes, hot compresses—have been shown to worsen tissue necrosis and delay healing.
The challenge, therefore, is to separate empirically harmful practices from potentially beneficial plant-based interventions, and to reframe traditional medicine as a supportive, regulated, and evidence-informed partner.
Medicinal Plants Used in the Supportive Management of Achaere
7.1 Azadirachta indica (Neem)
Neem is one of the most widely studied medicinal plants in tropical medicine. Its bioactive compounds—nimbidin, azadirachtin, quercetin—exhibit antibacterial, anti-inflammatory, and immunomodulatory properties.
Relevance to Achaere: Neem shows inhibitory effects against Mycobacterium species and common wound pathogens. Mild decoctions may be used for wound cleansing, provided they are non-caustic and sterile.
7.2 Vernonia amygdalina (Bitter Leaf)
A cornerstone of Igbo ethnomedicine, V. amygdalina contains sesquiterpene lactones and flavonoids with antimicrobial and antioxidant effects.
It is used primarily as oral immune support and metabolic modulation rather than direct ulcer application.
7.3 Psidium guajava (Guava Leaves)
Guava leaves possess strong antibacterial and astringent properties, effective against Staphylococcus aureus and Pseudomonas aeruginosa—key secondary invaders in chronic ulcers.
It has adjunct role in wound cleansing and exudate control.
7.4 Carica papaya (Pawpaw)
Papaya latex contains papain, a proteolytic enzyme used in enzymatic debridement.
It should be noted that while beneficial when standardized, crude latex may cause irritation and should not be applied indiscriminately.
7.5 Aloe vera
Aloe vera promotes epithelialization, reduces inflammation, and minimizes scar formation.
It is best suited for healing stages rather than active necrotic ulcers.
7.6 Curcuma longa (Turmeric)
Curcumin exhibits anti-inflammatory, antioxidant, and immune-modulatory properties.
Its application should be for oral supplementation; and raw powder should not be packed into ulcers.
7.7 Ocimum gratissimum (Nchuanwu / Scent Leaf)
Contains eugenol and thymol with antimicrobial activity.
It can be used for mild topical cleansing and general skin hygiene.
7.8 Medical-Grade Honey
Unlike raw honey, medical-grade honey is sterilized and standardized.
It has demonstrated broad-spectrum antimicrobial activity and accelerates wound healing.
Safety, Ethics, and Cultural Responsibility
The integration of medicinal plants into Buruli ulcer management must adhere to:
Non-maleficence
Standardization
Supervision
Clear communication that herbs are adjunctive
Ethically, healthcare providers must respect cultural beliefs while firmly discouraging harmful practices.
Proposed Integrative Model for Achaere Management
Early diagnosis and antibiotic therapy
Professional wound care
Selected herbal adjuncts with known safety profiles
Nutritional rehabilitation
Community education and surveillance
This model aligns biomedical efficacy with cultural relevance.
Future Research Directions
Phytochemical isolation of anti-mycolactone compounds
Toxicity profiling of commonly used herbs
Controlled clinical trials of adjunctive herbal therapies
Development of standardized African herbaceutical wound products
Conclusion
Achaere (Buruli ulcer) is neither mystical nor incurable. It is a bacterial disease whose devastation is amplified by delayed care and harmful interventions. African medicinal plants, when subjected to scientific scrutiny and ethical integration, hold value as supportive tools in comprehensive care. The future of Buruli ulcer management in Africa lies not in rejecting tradition, but in disciplining it with science.
Above all, every problem has a solution even at infinity.
Thanks and God bless.
Being text of lecture delivered at 2026 Annual Convention of 1992 Set, PCC Ihioma
By Livy-Elcon Emereonye
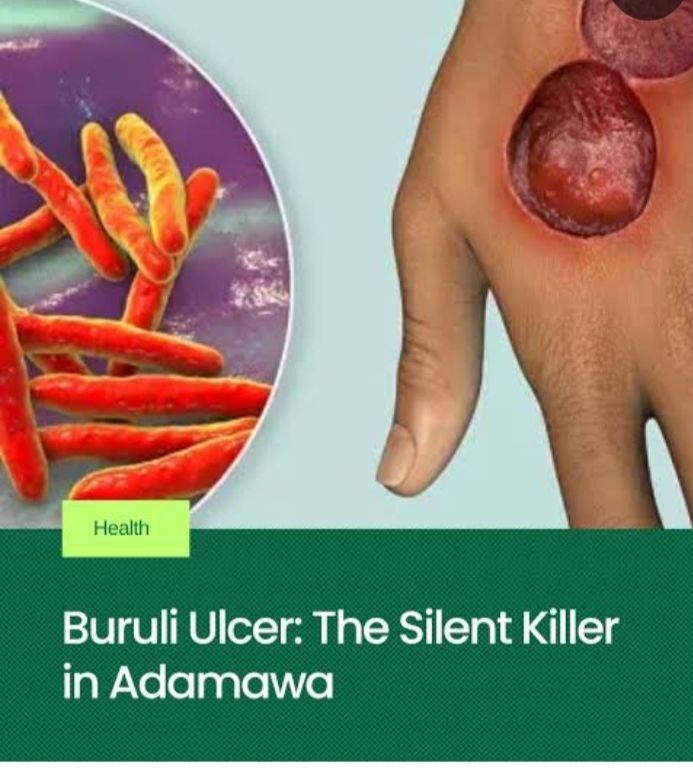
Buruli ulcer (BU), locally referred to in parts of Igboland as Achaere, is a neglected tropical disease caused by Mycobacterium ulcerans. Despite effective antibiotic regimens recommended by the World Health Organization (WHO), delayed presentation, sociocultural interpretations, and inappropriate traditional interventions continue to fuel high morbidity, deformity, and disability in endemic regions.
Introduction
Among the most severe but least addressed neglected tropical diseases (NTDs) is Buruli ulcer. Ranked after tuberculosis and leprosy among mycobacterial infections, BU disproportionately affects rural populations in West and Central Africa, including Nigeria, Ghana, Côte d’Ivoire, and Cameroon. In endemic Nigerian communities, particularly among the Igbo, the disease is colloquially known as Achaere, a term that often carries cultural, spiritual, or metaphysical interpretations.
These interpretations, though culturally meaningful, frequently delay biomedical intervention. Patients often present late, with advanced ulcers, secondary infection, bone involvement, and irreversible disability. At the same time, African traditional medicine remains the first line of care for many rural populations due to accessibility, affordability, and cultural trust.
This reality necessitates not a dismissal of traditional medicine, but a critical scientific engagement with it. The goal of this review is to examine medicinal plants traditionally used for Achaere, evaluate their evidence base, and propose a rational integrative framework that aligns ethnomedical knowledge with modern infectious disease management.
Epidemiology and Public Health Significance
Buruli ulcer is endemic in over 33 countries worldwide, with Africa accounting for the vast majority of cases. Children under 15 years constitute a significant proportion of patients, although adults are also affected. The disease is closely associated with riverine and swampy environments, agricultural activity, and limited access to healthcare.
In Nigeria, underreporting remains a major challenge. Many cases never reach hospitals, instead being managed in traditional settings until complications arise. This contributes to the perception that BU is incurable or spiritually driven, further entrenching harmful treatment practices.
Etiology and Pathophysiology
3.1 Causative Agent
Buruli ulcer is caused by Mycobacterium ulcerans, an environmental mycobacterium distinct from M. tuberculosis and M. leprae. Its unique pathogenicity lies in its production of mycolactone, a lipid toxin.
Mycobacterium ulcerans are rod-shaped, Gram positive bacteria that grow slowly, forming small transparent colonies after four weeks when viewed on a microscope.
Mosquitoes and other aquatic insects (like water bugs) are the primary vectors transmitting the ulcer-causing bacteria Mycobacterium ulcerans from the environment to people.
3.2 Role of Mycolactone
Mycolactone is a nasty toxin:
Induces apoptosis of skin and subcutaneous cells leading to ulcers and tissue damage.
Suppresses local immune responses
Explains the painless nature of early lesions
As a result, patients often ignore early nodules or plaques until extensive tissue destruction has occurred.
3.3 The Role of Immunity
In Buruli ulcer, immunity plays a crucial role:
The disease often affects people with weakened immune systems.
Research suggests that a strong cell-mediated immune response is key to controlling M. ulcerans infection.
Mycolactone suppresses the immune system, making it harder for the body to fight the infection.
Early treatment and a healthy immune system can improve outcomes.
Clinical Presentation
4.1 Early Lesions
Painless nodules
Firm plaques
Diffuse, non-pitting edema
4.2 Advanced Disease
Large ulcers with undermined edges
Necrosis of skin and subcutaneous tissue
Secondary bacterial infection
Osteomyelitis
Deformity and contractures
Pain typically appears late, often signaling secondary infection rather than primary disease activity.
WHO-recommended treatment consists of 8 weeks of combination antibiotic therapy, usually:
Rifampicin + Clarithromycin
This regimen achieves cure rates exceeding 90% when initiated early.
(or Rifampicin + Streptomycin in some settings)
Wound Care
Regular sterile dressing
Debridement of dead tissue
Skin grafting in advanced cases
Physiotherapy to prevent deformities
Psychosocial support.
Surgery
Reserved for large or complicated ulcers
Used alongside antibiotics, not alone
The Place of Traditional Medicine in Achaere
In many African communities, traditional medicine is not an alternative but the default healthcare system. However, in the context of Buruli ulcer, certain practices—scarification, caustic herbal pastes, hot compresses—have been shown to worsen tissue necrosis and delay healing.
The challenge, therefore, is to separate empirically harmful practices from potentially beneficial plant-based interventions, and to reframe traditional medicine as a supportive, regulated, and evidence-informed partner.
Medicinal Plants Used in the Supportive Management of Achaere
7.1 Azadirachta indica (Neem)
Neem is one of the most widely studied medicinal plants in tropical medicine. Its bioactive compounds—nimbidin, azadirachtin, quercetin—exhibit antibacterial, anti-inflammatory, and immunomodulatory properties.
Relevance to Achaere: Neem shows inhibitory effects against Mycobacterium species and common wound pathogens. Mild decoctions may be used for wound cleansing, provided they are non-caustic and sterile.
7.2 Vernonia amygdalina (Bitter Leaf)
A cornerstone of Igbo ethnomedicine, V. amygdalina contains sesquiterpene lactones and flavonoids with antimicrobial and antioxidant effects.
It is used primarily as oral immune support and metabolic modulation rather than direct ulcer application.
7.3 Psidium guajava (Guava Leaves)
Guava leaves possess strong antibacterial and astringent properties, effective against Staphylococcus aureus and Pseudomonas aeruginosa—key secondary invaders in chronic ulcers.
It has adjunct role in wound cleansing and exudate control.
7.4 Carica papaya (Pawpaw)
Papaya latex contains papain, a proteolytic enzyme used in enzymatic debridement.
It should be noted that while beneficial when standardized, crude latex may cause irritation and should not be applied indiscriminately.
7.5 Aloe vera
Aloe vera promotes epithelialization, reduces inflammation, and minimizes scar formation.
It is best suited for healing stages rather than active necrotic ulcers.
7.6 Curcuma longa (Turmeric)
Curcumin exhibits anti-inflammatory, antioxidant, and immune-modulatory properties.
Its application should be for oral supplementation; and raw powder should not be packed into ulcers.
7.7 Ocimum gratissimum (Nchuanwu / Scent Leaf)
Contains eugenol and thymol with antimicrobial activity.
It can be used for mild topical cleansing and general skin hygiene.
7.8 Medical-Grade Honey
Unlike raw honey, medical-grade honey is sterilized and standardized.
It has demonstrated broad-spectrum antimicrobial activity and accelerates wound healing.
Safety, Ethics, and Cultural Responsibility
The integration of medicinal plants into Buruli ulcer management must adhere to:
Non-maleficence
Standardization
Supervision
Clear communication that herbs are adjunctive
Ethically, healthcare providers must respect cultural beliefs while firmly discouraging harmful practices.
Proposed Integrative Model for Achaere Management
Early diagnosis and antibiotic therapy
Professional wound care
Selected herbal adjuncts with known safety profiles
Nutritional rehabilitation
Community education and surveillance
This model aligns biomedical efficacy with cultural relevance.
Future Research Directions
Phytochemical isolation of anti-mycolactone compounds
Toxicity profiling of commonly used herbs
Controlled clinical trials of adjunctive herbal therapies
Development of standardized African herbaceutical wound products
Conclusion
Achaere (Buruli ulcer) is neither mystical nor incurable. It is a bacterial disease whose devastation is amplified by delayed care and harmful interventions. African medicinal plants, when subjected to scientific scrutiny and ethical integration, hold value as supportive tools in comprehensive care. The future of Buruli ulcer management in Africa lies not in rejecting tradition, but in disciplining it with science.
Above all, every problem has a solution even at infinity.
Thanks and God bless.
An Integrative Medicine Approach to the Management of Achaere (Buruli Ulcer)
Being text of lecture delivered at 2026 Annual Convention of 1992 Set, PCC Ihioma
By Livy-Elcon Emereonye
Buruli ulcer (BU), locally referred to in parts of Igboland as Achaere, is a neglected tropical disease caused by Mycobacterium ulcerans. Despite effective antibiotic regimens recommended by the World Health Organization (WHO), delayed presentation, sociocultural interpretations, and inappropriate traditional interventions continue to fuel high morbidity, deformity, and disability in endemic regions.
Introduction
Among the most severe but least addressed neglected tropical diseases (NTDs) is Buruli ulcer. Ranked after tuberculosis and leprosy among mycobacterial infections, BU disproportionately affects rural populations in West and Central Africa, including Nigeria, Ghana, Côte d’Ivoire, and Cameroon. In endemic Nigerian communities, particularly among the Igbo, the disease is colloquially known as Achaere, a term that often carries cultural, spiritual, or metaphysical interpretations.
These interpretations, though culturally meaningful, frequently delay biomedical intervention. Patients often present late, with advanced ulcers, secondary infection, bone involvement, and irreversible disability. At the same time, African traditional medicine remains the first line of care for many rural populations due to accessibility, affordability, and cultural trust.
This reality necessitates not a dismissal of traditional medicine, but a critical scientific engagement with it. The goal of this review is to examine medicinal plants traditionally used for Achaere, evaluate their evidence base, and propose a rational integrative framework that aligns ethnomedical knowledge with modern infectious disease management.
Epidemiology and Public Health Significance
Buruli ulcer is endemic in over 33 countries worldwide, with Africa accounting for the vast majority of cases. Children under 15 years constitute a significant proportion of patients, although adults are also affected. The disease is closely associated with riverine and swampy environments, agricultural activity, and limited access to healthcare.
In Nigeria, underreporting remains a major challenge. Many cases never reach hospitals, instead being managed in traditional settings until complications arise. This contributes to the perception that BU is incurable or spiritually driven, further entrenching harmful treatment practices.
Etiology and Pathophysiology
3.1 Causative Agent
Buruli ulcer is caused by Mycobacterium ulcerans, an environmental mycobacterium distinct from M. tuberculosis and M. leprae. Its unique pathogenicity lies in its production of mycolactone, a lipid toxin.
Mycobacterium ulcerans are rod-shaped, Gram positive bacteria that grow slowly, forming small transparent colonies after four weeks when viewed on a microscope.
Mosquitoes and other aquatic insects (like water bugs) are the primary vectors transmitting the ulcer-causing bacteria Mycobacterium ulcerans from the environment to people.
3.2 Role of Mycolactone
Mycolactone is a nasty toxin:
Induces apoptosis of skin and subcutaneous cells leading to ulcers and tissue damage.
Suppresses local immune responses
Explains the painless nature of early lesions
As a result, patients often ignore early nodules or plaques until extensive tissue destruction has occurred.
3.3 The Role of Immunity
In Buruli ulcer, immunity plays a crucial role:
The disease often affects people with weakened immune systems.
Research suggests that a strong cell-mediated immune response is key to controlling M. ulcerans infection.
Mycolactone suppresses the immune system, making it harder for the body to fight the infection.
Early treatment and a healthy immune system can improve outcomes.
Clinical Presentation
4.1 Early Lesions
Painless nodules
Firm plaques
Diffuse, non-pitting edema
4.2 Advanced Disease
Large ulcers with undermined edges
Necrosis of skin and subcutaneous tissue
Secondary bacterial infection
Osteomyelitis
Deformity and contractures
Pain typically appears late, often signaling secondary infection rather than primary disease activity.
WHO-recommended treatment consists of 8 weeks of combination antibiotic therapy, usually:
Rifampicin + Clarithromycin
This regimen achieves cure rates exceeding 90% when initiated early.
(or Rifampicin + Streptomycin in some settings)
Wound Care
Regular sterile dressing
Debridement of dead tissue
Skin grafting in advanced cases
Physiotherapy to prevent deformities
Psychosocial support.
Surgery
Reserved for large or complicated ulcers
Used alongside antibiotics, not alone
The Place of Traditional Medicine in Achaere
In many African communities, traditional medicine is not an alternative but the default healthcare system. However, in the context of Buruli ulcer, certain practices—scarification, caustic herbal pastes, hot compresses—have been shown to worsen tissue necrosis and delay healing.
The challenge, therefore, is to separate empirically harmful practices from potentially beneficial plant-based interventions, and to reframe traditional medicine as a supportive, regulated, and evidence-informed partner.
Medicinal Plants Used in the Supportive Management of Achaere
7.1 Azadirachta indica (Neem)
Neem is one of the most widely studied medicinal plants in tropical medicine. Its bioactive compounds—nimbidin, azadirachtin, quercetin—exhibit antibacterial, anti-inflammatory, and immunomodulatory properties.
Relevance to Achaere: Neem shows inhibitory effects against Mycobacterium species and common wound pathogens. Mild decoctions may be used for wound cleansing, provided they are non-caustic and sterile.
7.2 Vernonia amygdalina (Bitter Leaf)
A cornerstone of Igbo ethnomedicine, V. amygdalina contains sesquiterpene lactones and flavonoids with antimicrobial and antioxidant effects.
It is used primarily as oral immune support and metabolic modulation rather than direct ulcer application.
7.3 Psidium guajava (Guava Leaves)
Guava leaves possess strong antibacterial and astringent properties, effective against Staphylococcus aureus and Pseudomonas aeruginosa—key secondary invaders in chronic ulcers.
It has adjunct role in wound cleansing and exudate control.
7.4 Carica papaya (Pawpaw)
Papaya latex contains papain, a proteolytic enzyme used in enzymatic debridement.
It should be noted that while beneficial when standardized, crude latex may cause irritation and should not be applied indiscriminately.
7.5 Aloe vera
Aloe vera promotes epithelialization, reduces inflammation, and minimizes scar formation.
It is best suited for healing stages rather than active necrotic ulcers.
7.6 Curcuma longa (Turmeric)
Curcumin exhibits anti-inflammatory, antioxidant, and immune-modulatory properties.
Its application should be for oral supplementation; and raw powder should not be packed into ulcers.
7.7 Ocimum gratissimum (Nchuanwu / Scent Leaf)
Contains eugenol and thymol with antimicrobial activity.
It can be used for mild topical cleansing and general skin hygiene.
7.8 Medical-Grade Honey
Unlike raw honey, medical-grade honey is sterilized and standardized.
It has demonstrated broad-spectrum antimicrobial activity and accelerates wound healing.
Safety, Ethics, and Cultural Responsibility
The integration of medicinal plants into Buruli ulcer management must adhere to:
Non-maleficence
Standardization
Supervision
Clear communication that herbs are adjunctive
Ethically, healthcare providers must respect cultural beliefs while firmly discouraging harmful practices.
Proposed Integrative Model for Achaere Management
Early diagnosis and antibiotic therapy
Professional wound care
Selected herbal adjuncts with known safety profiles
Nutritional rehabilitation
Community education and surveillance
This model aligns biomedical efficacy with cultural relevance.
Future Research Directions
Phytochemical isolation of anti-mycolactone compounds
Toxicity profiling of commonly used herbs
Controlled clinical trials of adjunctive herbal therapies
Development of standardized African herbaceutical wound products
Conclusion
Achaere (Buruli ulcer) is neither mystical nor incurable. It is a bacterial disease whose devastation is amplified by delayed care and harmful interventions. African medicinal plants, when subjected to scientific scrutiny and ethical integration, hold value as supportive tools in comprehensive care. The future of Buruli ulcer management in Africa lies not in rejecting tradition, but in disciplining it with science.
Above all, every problem has a solution even at infinity.
URGENT: MEDICAL NEGLIGENCE CRISIS DEMANDS IMMEDIATE OVERHAUL OF NIGERIA’S HEALTH REGULATORY FRAMEWORK
As a medical negligence legal specialist, I must express grave concern about the recurring incidents of absolutely preventable deaths resulting from medical negligence by health practitioners across Nigeria. The recent tragic loss of Nkanu Nnamdi, one of the twin sons of renowned author Chimamanda Ngozi Adichie and her husband, Dr. Ivara Esege, has once again brought this critical national crisis to the forefront of public consciousness.
As my professional focus over the last 20 years has been medical malpractice, having been involved in over 50 cases, this unfortunate incident is yet another example of the unacceptable state of incompetence in some Nigerian hospitals. I am, quite honestly, not shocked that such a simple procedure at an acclaimed, reputable hospital has ended so terribly. Propofol, which was reportedly administered to Nkanu, requires exceptional care due to its potential for cardio-respiratory failure. An overdose can be fatal, and there appears to be a strong possibility of overdose in this case.
I commend the Lagos State Government for its prompt commitment to investigate this matter. I equally commend the hospital, Euracare, for agreeing to cooperate with investigators. However, I must emphasise that such investigations must be genuinely independent and transparent. I have witnessed instances where medical records are altered to avoid culpability.
This issue is deeply personal to me. I was misdiagnosed for an ailment that could have had serious consequences. My brother almost died due to an operation performed by a physician who presented himself as a surgeon. The cases of Peju Ugboma and numerous other Nigerians—including a woman who lost both kidneys following negligent surgery; a mother who died from haemorrhagic shock after childbirth due to delayed response; a 12-year-old whose intestine reportedly went “missing” during treatment; a doctor who was imprisoned for improperly setting a fracture without X-ray; and an elderly woman who died after being mistakenly given a paralysing injection during a routine visit—demonstrate the scale of this crisis. These are not isolated incidents but symptoms of a systemic crisis demanding urgent intervention. My practice currently has over 20 complaints on this issue and is actively handling 25 cases.
The fundamental problem underlying these tragedies is the complete failure of the legal and regulatory framework governing Nigeria’s health sector. In the old days, the healthcare system functioned under a robust supervisory structure. Chief Medical Officers and Health Inspectors were responsible for oversight of critical care, ensuring compliance with standards, and holding practitioners accountable. The last Chief Medical Officer of Nigeria was Dr. Samuel Layinka Manuwa.
Today, under the National Health Act and State Health Laws, this essential regulatory infrastructure no longer exists. Our health sector has become overcentralised under the Federal Minister of Health, causing states to become lax in oversight responsibilities. As a result, health facilities and medical practitioners operate with alarming impunity. There is no requirement for routine submission of reports, no systematic inspections, and no effective enforcement of professional standards.
Ministers of Health and Commissioners of Health have assumed roles that conflate policy-making with regulatory enforcement—a fundamental governance failure. There must be a clear separation of functions: Ministers and Commissioners should focus on policy development and strategic direction, whilst independent Health Inspectors and regulatory bodies must be empowered to enforce standards, conduct inspections, and ensure accountability.
I commiserate with all Nigerians who have been victims of medical negligence and with families who continue to suffer the devastating consequences of a broken healthcare regulatory system. The Chimamanda case has brought this national emergency further into public focus, but it represents only the visible tip of a much larger crisis affecting countless Nigerian families. I continue to speak out as loudly as I can that the state of medical care in Nigeria has reached a critical point, requiring emergency action.
I call for:
Immediate establishment of an independent Health Regulatory Authority with powers to inspect facilities, enforce standards, and sanction non-compliance;
Reinstitution of the Office of Chief Medical Officer at federal and state levels with clear enforcement mandates;
Mandatory registration and periodic inspection of all health facilities with transparent reporting requirements;
Independent investigation mechanisms with powers to access and preserve medical records, preventing tampering or alteration;
Clear separation between policy formulation and regulatory enforcement within the health sector governance structure;
Comprehensive legislative reform to update Nigeria’s health laws to reflect modern standards of care, accountability, and patient protection; and
The time for comprehensive overhaul of Nigeria’s health system is long overdue. We cannot continue to lose precious lives to preventable medical errors whilst the regulatory framework remains in shambles. This is a matter of national emergency that demands immediate legislative and executive action.
DR. OLISA AGBAKOBA SAN SENIOR PARTNER & HEAD MEDICAL MALPRACTICE OLISA AGBAKOBA LEGAL
The National Agency for Food and Drug Administration and Control (NAFDAC) has called on the general public to be vigilant and report Adverse events or side effects related to the consumption of a sma infant formula across the Country
Ths public alert is coming amidst concerns arising from the voluntary global recall in over 50 countries by Nestlé UK of specific batches of its SMA Infant Formula and Follow-On Formula due to the potential presence of cereulide, a toxin, in the batches concerned.
The Agency in a media statement signed by the director general Professor Mojisola Adeyeye reassured the public, healthcare professionals, and relevant stakeholders particularly parents, and caregivers, that all Nestlé Infant Formulae currently approved for marketing in Nigeria are safe for consumption and are not part of the recalled batch.
The recall batches in the affected countries was due to the potential presence of cereulide in the UK batches, a toxin, which can trigger nausea and vomiting when consumed. Cereulide is an extremely heat-resistant toxin produced by certain strains of the bacterium Bacillus cereus.
According to the regulatory Agency ,The SMA range sold in Nigeria are manufactured at Nestlé Tuas Factory, Singapore, and duly registered with NAFDAC are as follows:
SMA GOLD 1 NAFDAC Reg. No.: B1-2783 SMA GOLD 2 NAFDAC Reg. No.: B1-2780 SMA GOLD 3 NAFDAC Reg. No.: B1-2781.
NAFDAC reiterated that the SMA and NAN range of infant formulae produced for the Nigerian market are not part of the affected batches involved in the voluntary and precautionary recall in other countries.
This alert has been issued as a precautionary measure in the interest of public health, consistent with NAFDACs statutory responsibility to keep Nigerians duly informed of emerging global food safety concerns, even in circumstances where the likelihood of local exposure remains minimal.